Each ZYPREXA 5 mg & 10 mg tablet contains 5 mg & 10mg, olanzapine respectively.
Each ZYPREXA ZYDIS 5 mg & 10 mg Orodispersible Tablet contains 5 mg and 10 mg olanzapine respectively.
Excipients/Inactive Ingredients: Zyprexa tab: Tablet core: Lactose monohydrate, Hydroxypropylcellulose, Crospovidone, Microcrystalline cellulose, Magnesium stearate.
Tablet 5 mg and 10 mg coat: Hypromellose, Color mixture white (hypromellose, titanium dioxide E171, macrogol, polysorbate 80), Carnauba wax, Edible blue ink (shellac, macrogol, indigo carmine E132).
Zyprexa Zydis orodispersible tab: Gelatin, Mannitol, Aspartame, Sodium methyl parahydroxybenzoate, Sodium propyl parahydroxybenzoate.
Pharmacotherapeutic group: psycholeptics, diazepines, oxazepines, thiazepines and oxepines. ATC code: N05A H03.
Pharmacology: Pharmacodynamics: Olanzapine is an antipsychotic, antimanic and mood stabilising agent that demonstrates a broad pharmacologic profile across a number of receptor systems.
In preclinical studies, olanzapine exhibited a range of receptor affinities (Ki; <100 nM) for serotonin 5 HT2A/2C, 5 HT3, 5 HT6; dopamine D1, D2, D3, D4, D5; cholinergic muscarinic receptors M1-M5; α1 adrenergic; and histamine H1 receptors. Animal behavioral studies with olanzapine indicated 5HT, dopamine, and cholinergic antagonism, consistent with the receptor-binding profile. Olanzapine demonstrated a greater in-vitro affinity for serotonin 5 HT2 than dopamine D2 receptors and greater 5 HT2 than D2 activity in vivo, models. Electrophysiological studies demonstrated that olanzapine selectively reduced the firing of mesolimbic (A10) dopaminergic neurons, while having little effect on the striatal (A9) pathways involved in motor function. Olanzapine reduced a conditioned avoidance response, a test indicative of antipsychotic activity, at doses below those producing catalepsy, an effect indicative of motor side-effects. Unlike some other antipsychotic agents, olanzapine increases responding in an "anxiolytic" test.
In a single oral dose (10 mg) Positron Emission tomography (PET) study in healthy volunteers, olanzapine produced a higher 5 HT2A than dopamine D2 receptor occupancy. In addition, a SPECT imaging study in schizophrenic patients revealed that olanzapine-responsive patients had lower striatal D2 occupancy than some other antipsychotic- and risperidone-responsive patients, while being comparable to clozapine-responsive patients.
Clinical efficacy: In two of two placebo and two of three comparator controlled trials with over 2,900 schizophrenic patients presenting with both positive and negative symptoms, olanzapine was associated with statistically significantly greater improvements in negative as well as positive symptoms. In a multinational, double-blind, comparative study of schizophrenia, schizoaffective, and related disorders which included 1,481 patients with varying degrees of associated depressive symptoms (baseline mean of 16.6 on the Montgomery-Asberg Depression Rating Scale), a prospective secondary analysis of baseline to endpoint mood score change demonstrated a statistically significant improvement (p= 0.001) favouring olanzapine (-6.0) versus haloperidol (-3.1).apine is not carcinogenic.
In patients with a manic or mixed episode of bipolar disorder, olanzapine demonstrated superior efficacy to placebo and valproate semisodium (divalproex) in reduction of manic symptoms over 3 weeks. Olanzapine also demonstrated comparable efficacy results to haloperidol in terms of the proportion of patients in symptomatic remission from mania and depression at 6 and 12 weeks. In a co-therapy study of patients treated with lithium or valproate for a minimum of 2 weeks, the addition of olanzapine 10 mg (co-therapy with lithium or valproate) resulted in a greater reduction in symptoms of mania than lithium or valproate monotherapy after 6 weeks.
In a 12-month recurrence prevention study in manic episode patients who achieved remission on olanzapine and were then randomised to olanzapine or placebo, olanzapine demonstrated statistically significant superiority over placebo on the primary endpoint of bipolar recurrence. Olanzapine also showed a statistically significant advantage over placebo in terms of preventing either recurrence into mania or recurrence into depression.
In a second 12-month recurrence prevention study in manic episode patients who achieved remission with a combination of olanzapine and lithium and were then randomised to olanzapine or lithium alone, olanzapine was statistically non-inferior to lithium on the primary endpoint of bipolar recurrence (olanzapine 30.0%, lithium 38.3%; p = 0.055).
In an 18-month co-therapy study in manic or mixed episode patients stabilised with olanzapine plus a mood stabiliser (lithium or valproate), long-term olanzapine co-therapy with lithium or valproate was not statistically significantly superior to lithium or valproate alone in delaying bipolar recurrence, defined according to syndromic (diagnostic) criteria.
Paediatric population: Controlled efficacy data in adolescents (ages 13 to 17 years) are limited to short term studies in schizophrenia (6 weeks) and mania associated with bipolar I disorder (3 weeks), involving less than 200 adolescents. Olanzapine was used as a flexible dose starting with 2.5 and ranging up to 20 mg/day. During treatment with olanzapine, adolescents gained significantly more weight compared with adults. The magnitude of changes in fasting total cholesterol, LDL cholesterol, triglycerides, and prolactin (see Precautions and Adverse Reactions) were greater in adolescents than in adults. There are no controlled data on maintenance of effect or long term safety (see Precautions and Adverse Reactions). Information on long term safety is primarily limited to open-label, uncontrolled data.
Further information on clinical trials: In a multinational, double-blind, comparative study of schizophrenia, schizoaffective, and related disorders which included 1,481 patients with varying degrees of associated depressive symptoms (baseline mean of 16.6 on the Montgomery-Asberg Depression Rating Scale), a prospective secondary analysis of baseline to endpoint mood score change demonstrated a statistically significant improvement (p=0.001) favouring olanzapine (-6.0) versus haloperidol (-3.1).
Pharmacokinetics: Olanzapine orodispersible tablet is bioequivalent to olanzapine coated tablets, with a similar rate and extent of absorption. Olanzapine orodispersible tablets may be used as an alternative to olanzapine coated tablets.
Absorption: Olanzapine is well absorbed after oral administration, reaching peak plasma concentrations within 5 to 8 hours. The absorption is not affected by food. Absolute oral bioavailability relative to intravenous administration has not been determined.
Distribution: The plasma protein binding of olanzapine was about 93 % over the concentration range of about 7 to about 1000 ng/ml. Olanzapine is bound predominantly to albumin and α1-acid-glycoprotein.
Biotransformation: Olanzapine is metabolized in the liver by conjugative and oxidative pathways. The major circulating metabolite is the 10-N-glucuronide, which does not pass the blood brain barrier. Cytochromes P450- CYP1A2 and P450-CYP2D6 contribute to the formation of the N-desmethyl and 2-hydroxymethyl metabolites, both exhibited significantly less in vivo pharmacological activity than olanzapine in animal studies. The predominant pharmacologic activity is from the parent olanzapine.
Elimination: After oral administration, the mean terminal elimination half-life of olanzapine in healthy subjects varied on the basis of age and gender.
In healthy elderly (65 and over) versus non-elderly subjects, the mean elimination half-life was prolonged (51.8 versus 33.8 hr) and the clearance was reduced (17.5 versus 18.2 l/hr). The pharmacokinetic variability observed in the elderly is within the range for the non-elderly. In 44 patients with schizophrenia > 65 years of age, dosing from 5 to 20 mg/day was not associated with any distinguishing profile of adverse events.
In female versus male subjects the mean elimination half life was somewhat prolonged (36.7 versus 32.3 hrs) and the clearance was reduced (18.9 versus 27.3 l/hr). However, olanzapine (5-20 mg) demonstrated a comparable safety profile in female (n=467) as in male patients (n=869).
Renal impairment: In renally impaired patients (creatinine clearance <10 ml/min) versus healthy subjects, there was no significant difference in mean elimination half-life (37.7 versus 32.4 hr) or clearance (21.2 versus 25.0 l/hr). A mass balance study showed that approximately 57 % of radiolabelled olanzapine appeared in urine, principally as metabolites.
Smokers: In smoking subjects with mild hepatic dysfunction, mean elimination half-life (39.3 hr) was prolonged and clearance (18.0 l/hr) was reduced analogous to non-smoking healthy subjects (48.8 hr and 14.1 l/hr, respectively).
In non-smoking versus smoking subjects (males and females) the mean elimination half-life was prolonged (38.6 versus 30.4 hr) and the clearance was reduced (18.6 versus 27.7 l/hr). The plasma clearance of olanzapine is lower in elderly versus young subjects, in females versus males, and in non-smokers versus smokers. However, the magnitude of the impact of age, gender, or smoking on olanzapine clearance and half-life is small in comparison to the overall variability between individuals.
In a study of Caucasians, Japanese, and Chinese subjects, there were no differences in the pharmacokinetic parameters among the three populations.
Paediatric population: Adolescents (ages 13 to 17 years): The pharmacokinetics of olanzapine are similar between adolescents and adults. In clinical studies, the average olanzapine exposure was approximately 27% higher in adolescents. Demographic differences between the adolescents and adults include a lower average body weight and fewer adolescents were smokers. Such factors possibly contribute to the higher average exposure observed in adolescents.
Toxicology: Preclinical safety data: Acute (single-dose) toxicity: Signs of oral toxicity in rodents were characteristic of potent neuroleptic compounds: hypoactivity, coma, tremors, clonic convulsions, salivation, and depressed weight gain. The median lethal doses were approximately 210 mg/kg (mice) and 175 mg/kg (rats). Dogs tolerated single oral doses up to 100 mg/kg without mortality. Clinical signs included sedation, ataxia, tremors, increased heart rate, labored respiration, miosis, and anorexia. In monkeys, single oral doses up to 100 mg/kg resulted in prostration and, at higher doses, semi-consciousness.
Repeated-dose toxicity: In studies up to 3 months duration in mice and up to 1 year in rats and dogs, the predominant effects were CNS depression, anticholinergic effects, and peripheral haematological disorders. Tolerance developed to the CNS depression. Growth parameters were decreased at high doses. Reversible effects consistent with elevated prolactin in rats included decreased weights of ovaries and uterus and morphologic changes in vaginal epithelium and in mammary gland.
Haematologic toxicity: Effects on haematology parameters were found in each species, including dose-related reductions in circulating leukocytes in mice and non-specific reductions of circulating leukocytes in rats; however, no evidence of bone marrow cytotoxicity was found. Reversible neutropenia, thrombocytopenia, or anaemia developed in a few dogs treated with 8 or 10 mg/kg/day (total olanzapine exposure [area under the curve] is 12- to 15-fold greater than that of a man given a 12-mg dose). In cytopenic dogs, there were no adverse effects on progenitor and proliferating cells in the bone marrow.
Reproductive toxicity: Olanzapine had no teratogenic effects. Sedation affected mating performance of male rats. Estrous cycles were affected at doses of 1.1 mg/kg (3 times the maximum human dose) and reproduction parameters were influenced in rats given 3 mg/kg (9 times the maximum human dose). In the offspring of rats given olanzapine, delays in foetal development and transient decreases in offspring activity levels were seen.
Mutagenicity: Olanzapine was not mutagenic or clastogenic in a full range of standard tests, which included bacterial mutation tests and in vitro and in vivo mammalian tests.
Carcinogenicity: Based on the results of studies in mice and rats, it was concluded that olanzapine is not carcinogenic.
Olanzapine is indicated for the treatment of schizophrenia.
Olanzapine is effective in maintaining the clinical improvement during continuing therapy in patients who have shown initial treatment response.
Olanzapine is indicated for short-term treatment of acute manic episode associated with Bipolar I Disorder.
Olanzapine is indicated for preventing recurrence of manic, mixed or depressive episodes in Bipolar I Disorder.
Adults: Schizophrenia: The recommended starting dose for olanzapine is 10 mg/day.
Manic episode: The starting dose is 15 mg as a single daily dose in monotherapy or 10 mg daily in combination therapy (See Pharmacology: Pharmacodynamics under Actions).
Preventing recurrence in bipolar disorder: The recommended starting dose is 10mg/day. For patients who have been receiving olanzapine for treatment of manic episode, continue therapy for preventing recurrence at the same dose. If a new manic, mixed, or depressive episode occurs, olanzapine treatment should be continued (with dose optimisation as needed), with supplementary therapy to treat mood symptoms, as clinically indicated.
During treatment for schizophrenia, manic episode and recurrence prevention in bipolar disorder, daily dosage may subsequently be adjusted on the basis of individual clinical status within the range 5-20 mg/day. An increase to a dose greater than the recommended starting dose is advised only after appropriate clinical reassessment and should generally occur at intervals of not less than 24 hours. Olanzapine can be given without regards for meals as absorption is not affected by food. Gradual tapering of the dose should be considered when discontinuing olanzapine.
Olanzapine orodispersible tablet should be placed in the mouth, where it will rapidly disperse in saliva, so it can be easily swallowed. Removal of the intact orodispersible tablet from the mouth is difficult. Since the orodispersible tablet is fragile, it should be taken immediately on opening the blister. Alternatively, it may be dispersed in a full glass of water or other suitable beverage (orange juice, apple juice, milk or coffee) immediately before administration.
Olanzapine orodispersible tablet is bioequivalent to olanzapine coated tablets, with a similar rate and extent of absorption. It has the same dosage and frequency of administration as olanzapine coated tablets. Olanzapine orodispersible tablets may be used as an alternative to olanzapine coated tablets.
Special populations: Elderly: A lower starting dose (5 mg/day) is not routinely indicated but should be considered for those 65 and over when clinical factors warrant (see Precautions).
Renal and/or hepatic impairment: A lower starting dose (5 mg) should be considered for such patients. In cases of moderate hepatic insufficiency (cirrhosis, Child-Pugh Class A or B), the starting dose should be 5 mg and only increased with caution.
Smokers: The starting dose and dose range need not be routinely altered for non-smokers relative to smokers. The metabolism of olanzapine may be induced by smoking. Clinical monitoring is recommended and an increase of olanzapine dose may be considered if necessary (see Interactions).
When more than one factor is present which might result in slower metabolism (female gender, geriatric age, non-smoking status), consideration should be given to decreasing the starting dose. Dose escalation, when indicated, should be conservative in such patients.
In cases where dose increments of 2.5 mg are considered necessary, ZYPREXA coated tablets should be used. (See Pharmacology: Pharmacokinetics under Actions and Interactions.)
Paediatric population: Olanzapine is not recommended for use in children and adolescents below 18 years of age due to a lack of data on safety and efficacy. A greater magnitude of weight gain, lipid and prolactin alterations has been reported in short term studies of adolescent patients than in studies of adult patients (see Pharmacology: Pharmacokinetics under Actions, Precautions and Adverse Reactions).
Signs and Symptoms: Very common symptoms in overdose (>10% incidence) include tachycardia, agitation/aggressiveness, dysarthria, various extrapyramidal symptoms, and reduced level of consciousness ranging from sedation to coma.
Other medically significant sequelae of overdose include delirium, convulsion, coma, possible neuroleptic malignant syndrome, respiratory depression, aspiration, hypertension or hypotension, cardiac arrhythmias (<2% of overdose cases) and cardiopulmonary arrest. Fatal outcomes have been reported for acute overdoses as low as 450 mg but survival has also been reported following acute overdose of approximately 2 g of oral olanzapine.
Treatment: There is no specific antidote for olanzapine. Induction of emesis is not recommended. Standard procedures for management of overdose maybe indicated (i.e. gastric lavage, administration of activated charcoal). The concomitant administration of activated charcoal was shown to reduce the oral bioavailability of olanzapine by 50 to 60%.
Symptomatic treatment and monitoring of vital organ function should be instituted according to clinical presentation, including treatment of hypotension and circulatory collapse and support of respiratory function. Do not use epinephrine, dopamine, or other sympathomimetic agents with beta-agonist activity since beta stimulation may worsen hypotension. Cardiovascular monitoring is necessary to detect possible arrhythmias. Close medical supervision and monitoring should continue until the patient recovers.
Hypersensitivity to the active substance or to any of the excipients listed in Description. Patients with known risk of narrow-angle glaucoma.
During antipsychotic treatment, improvement in the patient's clinical condition may take several days to some weeks. Patients should be closely monitored during this period.
Dementia-related psychosis and/or behavioural disturbances: Olanzapine is not recommended for use in patients with dementia-related psychosis and/or behavioural disturbances because of an increase in mortality and the risk of cerebrovascular accident. In placebo-controlled clinical trials (6-12 weeks duration) of elderly patients (mean age 78 years) with dementia-related psychosis and/or disturbed behaviours, there was a 2-fold increase in the incidence of death in olanzapine-treated patients compared to patients treated with placebo (3.5% vs. 1.5 %, respectively). The higher incidence of death was not associated with olanzapine dose (mean daily dose 4.4 mg) or duration of treatment. Risk factors that may predispose this patient population to increased mortality include age > 65 years, dysphagia, sedation, malnutrition and dehydration, pulmonary conditions (e.g., pneumonia, with or without aspiration), or concomitant use of benzodiazepines. However, the incidence of death was higher in olanzapine-treated than in placebo- treated patients independent of these risk factors.
In the same clinical trials, cerebrovascular adverse events (CVAE e.g., stroke, transient ischemic attack), including fatalities, were reported. There was a 3-fold increase in CVAE in patients treated with olanzapine compared to patients treated with placebo (1.3 % vs. 0.4 %, respectively). All olanzapine- and placebo-treated patients who experienced a cerebrovascular event had pre-existing risk factors. Age > 75 years and vascular/mixed type dementia were identified as risk factors for CVAE in association with olanzapine treatment. The efficacy of olanzapine was not established in these trials.
Parkinson's disease The use of olanzapine in the treatment of dopamine agonist associated psychosis in patients with Parkinson's disease is not recommended. In clinical trials, worsening of Parkinsonian symptomatology and hallucinations were reported very commonly and more frequently than with placebo (see Adverse Reactions), and olanzapine was not more effective than placebo in the treatment of psychotic symptoms. In these trials, patients were initially required to be stable on the lowest effective dose of anti- Parkinsonian medicinal products (dopamine agonist) and to remain on the same anti-Parkinsonian medicinal products and dosages throughout the study. Olanzapine was started at 2.5 mg/day and titrated to a maximum of 15 mg/day based on investigator judgement.
Neuroleptic Malignant Syndrome (NMS): NMS is a potentially life-threatening condition associated with antipsychotic medicinal products. Rare cases reported as NMS have also been received in association with olanzapine. Clinical manifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status, and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia). Additional signs may include elevated creatine phosphokinase, myoglobinuria (rhabdomyolysis), and acute renal failure. If a patient develops signs and symptoms indicative of NMS, or presents with unexplained high fever without additional clinical manifestations of NMS, all antipsychotic medicines, including olanzapine must be discontinued.
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) has been reported with olanzapine exposure. DRESS consists of a combination of three or more of the following: cutaneous reaction (such as rash or exfoliative dermatitis), eosinophilia, fever, lymphadenopathy and one or more systemic complications such as hepatitis, nephritis, pneumonitis, myocarditis, and pericarditis. Discontinue olanzapine if DRESS is suspected.
Hyperglycaemia and diabetes: Hyperglycaemia in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients treated with atypical antipsychotics. Assessment of the relationship between atypical antipsychotics use and glucose abnormalities is complicated by the possibility of an increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population. Given this confounders, the relationship between atypical antipsychotic use and hyperglycaemiarelated adverse events is not completely understood. However, epidemiological studies suggest an increased risk of treatment-emergent hyperglycaemia-related adverse events in patients treated with the atypical antipsychotics. Precise risk estimates for hyperglycaemia-related adverse events in patients treated with atypical antipsychotics are not available.
Patients with an established diagnosis of diabetes mellitus who are started on atypical antipsychotics should be monitored regularly for worsening of glucose control. Patients with risk factors for diabetes mellitus (e.g. obesity, family history of diabetes) who are starting treatment with atypical antipsychotics should undergo fasting blood glucose testing at the beginning of treatment and periodically during treatment. Any patient treated with atypical antipsychotics should be monitored for symptoms of hyperglycemia including polydipsia, polyuria, polyphagia, and weakness. Patients who develop symptoms of hyperglycemia during treatment with atypical antipsychotics should undergo fasting blood glucose testing. In some cases, hyperglycaemia has resolved when the atypical antipsychotic was discontinued; however, some patients required continuation of anti-diabetic treatment despite discontinuation of the suspect drug.
Lipid alterations: Undesirable alterations in lipids have been observed in olanzapine-treated patients in placebocontrolled clinical trials (seeAdverse Reactions). Lipid alterations should be managed as clinically appropriate, particularly in dyslipidemic patients and in patients with risk factors for the development of lipids disorders. Patients treated with any antipsychotic medicines, including ZYPREXA and ZYPREXA ZYDIS, should be monitored regularly for lipids in accordance with utilised antipsychotic guidelines, e.g. at baseline, 12 weeks after starting olanzapine treatment and every 5 years thereafter.
Anticholinergic activity: While olanzapine demonstrated anticholinergic activity in vitro, experience during the clinical trials revealed a low incidence of related events. However, as clinical experience with olanzapine in patients with concomitant illness is limited, caution is advised when prescribing for patients with prostatic hypertrophy, or paralytic ileus and related conditions.
Hepatic function: Transient, asymptomatic elevations of hepatic aminotransferases, ALT, AST have been seen commonly, especially in early treatment. Caution should be exercised and follow-up organised in patients with elevated ALT and/or AST, in patients with signs and symptoms of hepatic impairment, in patients with pre-existing conditions associated with limited hepatic functional reserve, and in patients who are being treated with potentially hepatotoxic medicines. In cases where hepatitis (including hepatocellular, cholestatic or mixed liver injury) has been diagnosed, olanzapine treatment should be discontinued.
Neutropenia: Caution should be exercised in patients with low leukocyte and/or neutrophil counts for any reason, in patients receiving medicines known to cause neutropenia, in patients with a history of drug-induced bone marrow depression/toxicity, in patients with bone marrow depression caused by concomitant illness, radiation therapy or chemotherapy and in patients with hypereosinophilic conditions or with myeloproliferative disease. Neutropenia has been reported commonly when olanzapine and valproate are used concomitantly (see Adverse Reactions).
Discontinuation of treatment: Acute symptoms such as sweating, insomnia, tremor, anxiety, nausea, or vomiting have been reported rarely (≥ 0.01 % and < 0.1 %) when olanzapine is stopped abruptly.
QT interval: In clinical trials, clinically meaningful QTc prolongations (Fridericia QT correction [QTcF] ≥ 500 milliseconds [msec] at any time post baseline in patients with baseline QTcF < 500 msec) were uncommon (0.1 % to 1 %) in patients treated with olanzapine, with no significant differences in associated cardiac events compared to placebo. However, caution should be exercised when olanzapine is prescribed with medicines known to increase QTc interval, especially in the elderly, in patients with congenital long QT syndrome, congestive heart failure, heart hypertrophy, hypokalaemia or hypomagnesaemia.
Thromboembolism: Temporal association of olanzapine treatment and venous thromboembolism has been reported uncommonly (≥ 0.1% and < 1%). A causal relationship between the occurrence of venous thromboembolism and treatment with olanzapine has not been established. However, since patients with schizophrenia often present with acquired risk factors for venous thromboembolism all possible risk factors of VTE e.g. immobilisation of patients, should be identified and preventive measures undertaken.
General CNS activity: Given the primary CNS effects of olanzapine, caution should be used when it is taken in combination with other centrally acting medicines and alcohol. As it exhibits in vitro dopamine antagonism, olanzapine may antagonize the effects of direct and indirect dopamine agonists.
Seizures: Olanzapine should be used cautiously in patients who have a history of seizures or are subject to factors which may lower the seizure threshold. Seizures have been reported to occur uncommonly in patients when treated with olanzapine. In most of these cases, a history of seizures or risk factors for seizures were reported.
Tardive Dyskinesia: In comparator studies of one year or less duration, olanzapine was associated with a statistically significant lower incidence of treatment emergent dyskinesia. However the risk of tardive dyskinesia increases with long term exposure, and therefore if signs or symptoms of tardive dyskinesia appear in a patient on olanzapine, a dose reduction or discontinuation should be considered. These symptoms can temporally deteriorate or even arise after discontinuation of treatment.
Postural hypotension: Postural hypotension was infrequently observed in the elderly in olanzapine clinical trials. It is recommended that blood pressure is measured periodically in patients over 65 years.
Sudden cardiac death: In postmarketing reports with olanzapine, the event of sudden cardiac death has been reported in patients with olanzapine. In a retrospective observational cohort study, the risk of presumed sudden cardiac death in patients treated with olanzapine was approximately twice the risk in patients not using antipsychotics. In the study, the risk of olanzapine was comparable to the risk of atypical antipsychotics included in a pooled analysis.
Paediatric population: Olanzapine is not indicated for use in the treatment of children and adolescents. Studies in patients aged 13-17 years showed various adverse reactions, including weight gain, changes in metabolic parameters and increases in prolactin levels(see Pharmacology: Pharmacodynamics under Actions and Adverse Reactions).
Lactose: ZYPREXA tablets contain lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Phenylalanine: ZYPREXA ZYDIS Orodispersible Tablet contains aspartame, which is a source of phenylalanine. May be harmful for people with phenylketonuria.
Mannitol: ZYPREXA ZYDIS Orodispersible Tablet contains mannitol.
Sodium methyl parahydroxybenzoate and sodium propyl parahydroxybenzoate: Olanzapine orodispersible tablet contains sodium methyl parahydroxybenzoate and sodium propyl parahydroxybenzoate. These preservatives are known to cause urticaria. Generally, delayed type reactions such as contact dermatitis may occur, but rarely immediate reactions with bronchospasm may occur.
Effects on ability to drive and use machines: No studies on the effects on the ability to drive and use machines have been performed. Because olanzapine may cause somnolence and dizziness, patients should be cautioned about operating machinery, including motor vehicles.
Pregnancy: There are no adequate and well-controlled studies in pregnant women. Patients should be advised to notify their physician if they become pregnant or intend to become pregnant during treatment with olanzapine.
Neonates exposed to antipsychotic drugs during the third trimester of pregnancy are at risk for extrapyramidal and/or withdrawal symptoms following delivery. There have been reports of agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress and feeding disorder in these neonates. These complications have varied in severity; while in some cases symptoms have been self-limited, in other cases neonates have required intensive care unit support and prolonged hospitalization.
ZYPREXA and ZYPREXA ZYDIS should be used during pregnancy only if the potential benefit justifies the potential risk to the foetus.
Breast-feeding: In a study in breast-feeding, healthy women, olanzapine was excreted in breast milk. Mean infant exposure (mg/kg) at steady state was estimated to be 1.8 % of the maternal olanzapine dose (mg/kg). Patients should be advised not to breast feed an infant if they are taking olanzapine.
Fertility: Effects on fertility are unknown (see Pharmacology: Toxicology: Preclinical safety data under Actions for preclinical information).
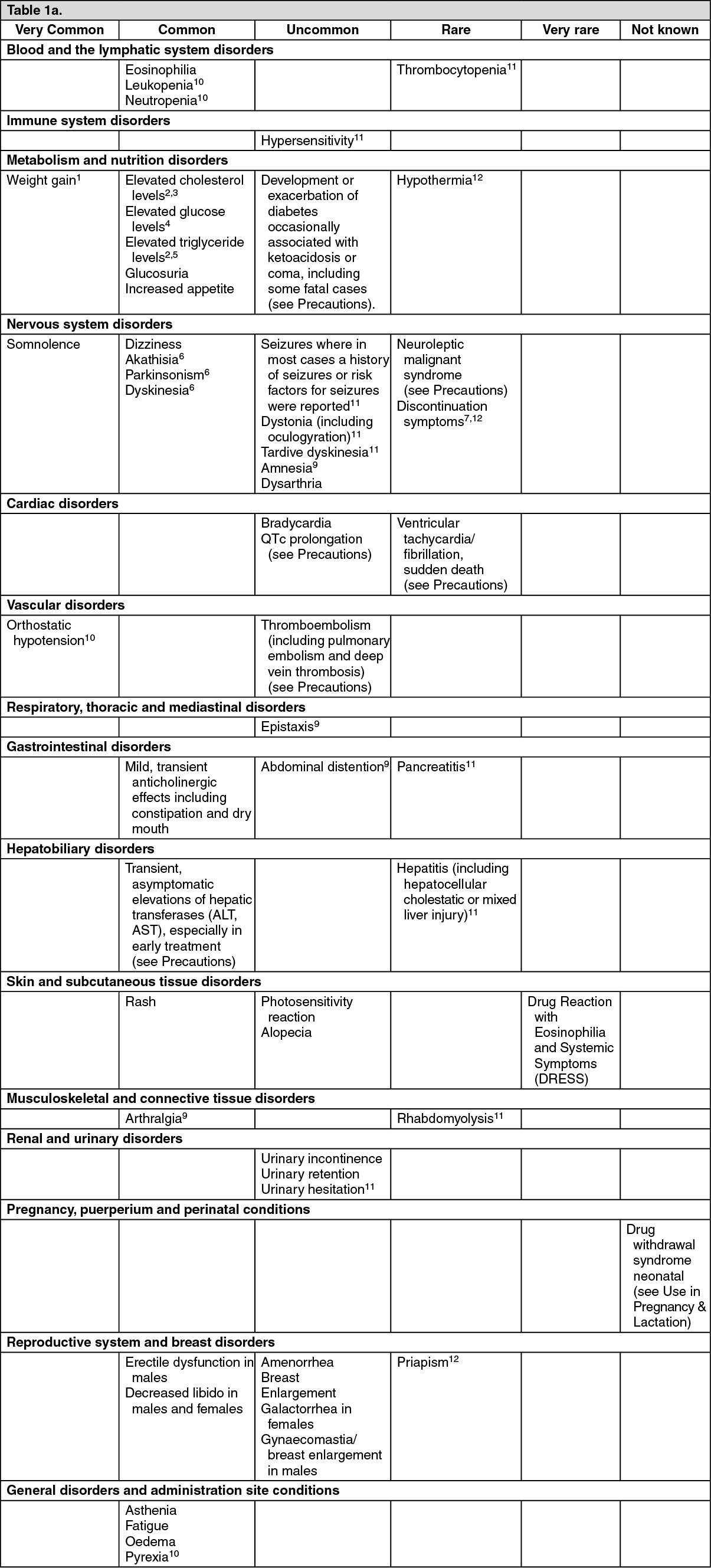
Summary of the safety profile: Adults: The most frequently (seen in ≥ 1% of patients ) reported adverse reactions associated with the use of olanzapine in clinical trials were somnolence, weight gain, eosinophilia, elevated prolactin, cholesterol, glucose and triglyceride levels (see section 4.4), glucosuria, increased appetite, dizziness, akathisia, parkinsonism, leukopenia, neutropenia (see Precautions), dyskinesia, orthostatic hypotension, anticholinergic effects, transient asymptomatic elevations of hepatic aminotransferases (see Precautions), rash, asthenia, fatigue, pyrexia, arthralgia, increased alkaline phosphatase, high gamma glutamyltransferase, high uric acid, high creatine phosphokinase and oedema.
Tabulated list of adverse reactions: The following table lists the adverse reactions and laboratory investigations observed from spontaneous reporting and in clinical trials. Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. The frequency terms listed are defined as follows: Very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to< 1/1,000), very rare (< 1/10,000), not known (cannot be estimated from the data available). (See Table 1A and Table 1B.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Long-term exposure (at least 48 weeks): The proportion of patients who had adverse, clinically significant changes in weight gain, glucose, total/LDL/HDL cholesterol or triglycerides increased over time. In adult patients who completed 9-12 months of therapy, the rate of increase in mean blood glucose slowed after approximately 6 months.
Additional information on special populations: In clinical trials in elderly patients with dementia, olanzapine treatment was associated with a higher incidence of death and cerebrovascular adverse reactions compared to placebo (see Precautions). Very common adverse reactions associated with the use of olanzapine in this patient group were abnormal gait and falls. Pneumonia, increased body temperature, lethargy, erythema, visual hallucinations and urinary incontinence were observed commonly.
In clinical trials in patients with drug-induced (dopamine agonist) psychosis associated with Parkinson’s disease, worsening of Parkinsonian symptomatology and hallucinations were reported very commonly and more frequently than with placebo.
In one clinical trial in patients with bipolar mania, valproate combination therapy with olanzapine resulted in an incidence of neutropenia of 4.1%; a potential contributing factor could be high plasma valproate levels. Olanzapine administered with lithium or valproate resulted in increased levels (≥10%) of tremor, dry mouth, increased appetite, and weight gain. Speech disorder was also reported commonly. During treatment with olanzapine in combination with lithium or divalproex, an increase of ≥ 7% from baseline body weight occurred in 17.4% of patients during acute treatment (up to 6 weeks). Long-term olanzapine treatment (up to 12 months) for recurrence prevention in patients with bipolar disorder was associated with an increase of ≥7% from baseline body weight in 39.9% of patients.
Paediatric population: Olanzapine is not indicated for the treatment of children and adolescent patients below 18 years. Although no clinical studies designed to compare adolescents to adults have been conducted, data from the adolescent trials were compared to those of the adult trials.
The following table summarises the adverse reactions reported with a greater frequency in adolescent patients (aged 13-17 years) than in adult patients or adverse reactions only identified during short- term clinical trials in adolescent patients. Clinically significant weight gain (≥ 7%) appears to occur more frequently in the adolescent population compared to adults with comparable exposures. The magnitude of weight gain and the proportion of adolescent patients who had clinically significant weight gain were greater with long-term exposure (at least 24 weeks) than with short-term exposure.
Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. The frequency terms listed are defined as follows: Very common (≥ 1/10), common (≥ 1/100 to < 1/10). (See Table 2.)
Click on icon to see table/diagram/image
Interaction studies have only been performed in adults.
Potential interactions affecting olanzapine: Since olanzapine is metabolised by CYP1A2, substances that can specifically induce or inhibit this isoenzyme may affect the pharmacokinetics of olanzapine.
Induction of CYP1A2: The metabolism of olanzapine may be induced by smoking and carbamazepine, which may lead to reduced olanzapine concentrations. Only slight to moderate increase in olanzapine clearance has been observed. The clinical consequences are likely to be limited, but clinical monitoring is recommended and an increase of olanzapine dose may be considered if necessary (see Dosage & Administration).
Inhibition of CYP1A2: Fluvoxamine, a specific CYP1A2 inhibitor, has been shown to significantly inhibit the metabolism of olanzapine. The mean increase in olanzapine Cmax following fluvoxamine was 54 % in female non- smokers and 77 % in male smokers. The mean increase in olanzapine AUC was 52 % and 108 % respectively. A lower starting dose of olanzapine should be considered in patients who are using fluvoxamine or any other CYP1A2 inhibitors, such as ciprofloxacin. A decrease in the dose of olanzapine should be considered if treatment with an inhibitor of CYP1A2 is initiated.
Decreased bioavailability: Activated charcoal reduces the bioavailability of oral olanzapine by 50 to 60 % and should be taken at least 2 hours before or after olanzapine.
Fluoxetine (a CYP2D6 inhibitor), single doses of antacid (aluminium, magnesium) or cimetidine have not been found to significantly affect the pharmacokinetics of olanzapine.
Potential for olanzapine to affect other medicinal products: Olanzapine may antagonise the effects of direct and indirect dopamine agonists.
Olanzapine does not inhibit the main CYP450 isoenzymes in vitro (e.g. 1A2, 2D6, 2C9, 2C19, 3A4). Thus no particular interaction is expected as verified through in vivo studies where no inhibition of metabolism of the following active substances was found: tricyclic antidepressant (representing mostly CYP2D6 pathway), warfarin (CYP2C9), theophylline (CYP1A2) or diazepam (CYP3A4 and 2C19).
Olanzapine showed no interaction when co-administered with lithium or biperiden.
Therapeutic monitoring of valproate plasma levels did not indicate that valproate dosage adjustment is required after the introduction of concomitant olanzapine.
General CNS activity: Caution should be exercised in patients who consume alcohol or receive medicinal products that can cause central nervous system depression. The concomitant use of olanzapine with anti-Parkinsonian medicinal products in patients with Parkinson's disease and dementia is not recommended (see Precautions).
QTc interval: Caution should be used if olanzapine is being administered concomitantly with medicinal products known to increase QTc interval (see Precautions).
Special precautions for disposal: No special requirements.
Incompatibilities: Not applicable.
ZYPREXA tab: Store at 25°C in the original package.
ZYPREXA ZYDIS orodispersible tab: Store below 30°C in the original package.
Shelf-Life: ZYPREXA tab & Zyprexa Zydis orodispersible tab: 3 years when stored under appropriate conditions.
N05AH03 - olanzapine ; Belongs to the class of diazepines, oxazepines and thiazepines antipsychotics
Zyprexa Zydis orodispersible tab 10 mg
28's
Zyprexa Zydis orodispersible tab 5 mg
28's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image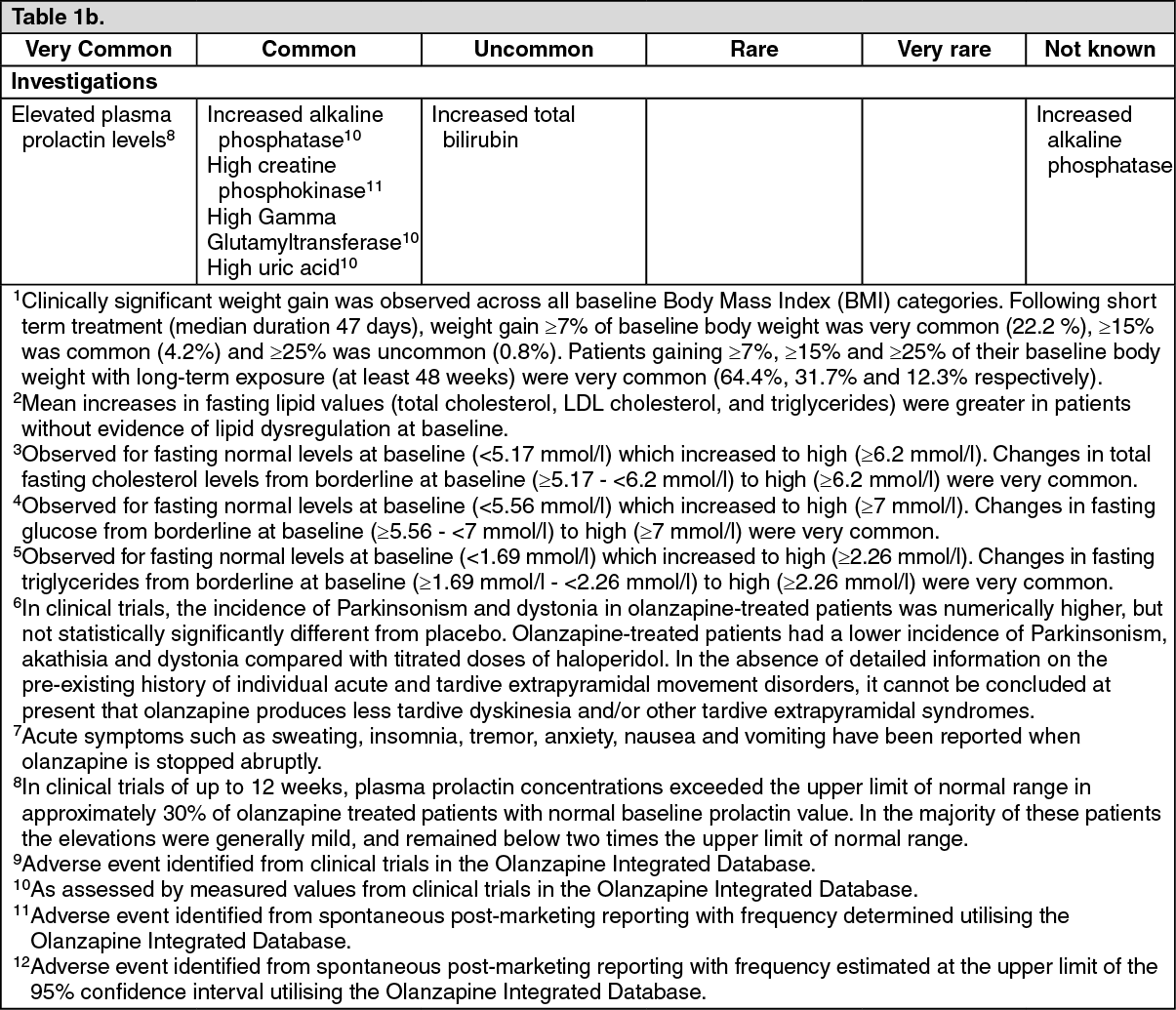 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image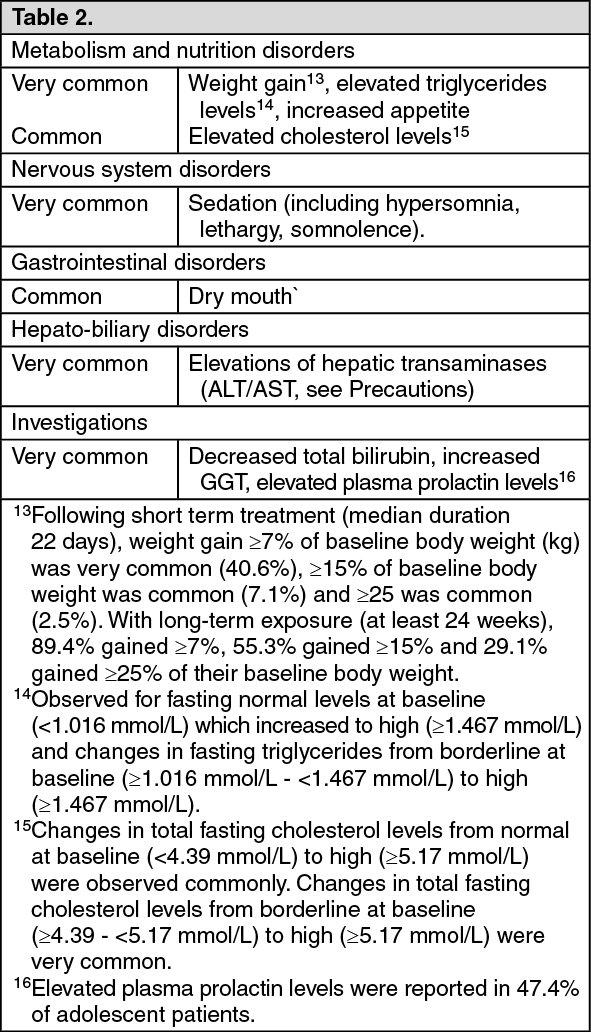 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
